- Treatment of bradycardia
Atropine
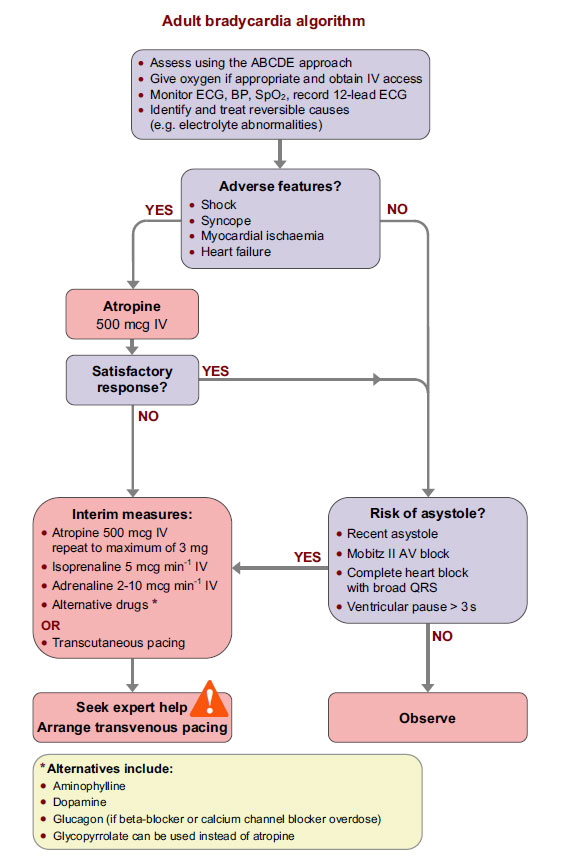
As detailed in the bradycardia algorithm (available from the algorithm tab), where there are adverse features, give 500 mcg of atropine intravenously.
If there is not a satisfactory response, this dosage of atropine can be repeated up to a maximum total does of 3 mg.
Other options for drug treatment are listed in the algorithm. Alternatively, transcutaneous pacing may be used.
Cardiac pacing
In some cardiac arrest or peri-arrest settings, appropriate use of cardiac pacing can be life-saving.
Non-invasive pacing may be used to maintain cardiac output temporarily while expert help to deliver longer-term treatment is obtained. Non-invasive pacing can be established rapidly and is well within the capabilities of an ALS provider.
Cardiac pacemakers
The ALS provider does not need to have a detailed technical knowledge of permanent cardiac pacemakers and implanted cardioverter defibrillators (ICDs) but needs to be able to recognise:
- When one of these devices is present
- When they are failing
- How the presence of an implanted device may influence the management of a cardiac arrest.
Implanted devices that deliver pacing include pacemakers implanted for the treatment of bradycardia, as well as ICDs (which have pacing capacity) and biventricular pacemakers (implanted for left ventricular failure).
Percussion pacing
When bradycardia is so profound that it causes clinical cardiac arrest, percussion pacing may be used in preference to CPR because it may produce an adequate cardiac output with less trauma to the patient.
To perform percussion pacing:
- With the side of a closed fist deliver repeated firm blows to the precordium lateral to the lower left sternal edge.
- Raise the hand about 10 cm above the chest for each blow.
- If initial blows do not produce a QRS complex try using slightly harder blows and try moving the point of contact around the precordium until a site is found that produces repeated ventricular stimulation.
If attempted percussion pacing does not achieve a cardiac output within a few seconds, start CPR.
Transcutaneous pacing
Patients requiring transcutaneous pacing are likely to need sedation. Transcutaneous pacing and drugs used in extreme bradycardia should be a bridge to definitive treatment (transvenous pacing and/or correction of the cause of the extreme bradycardia).
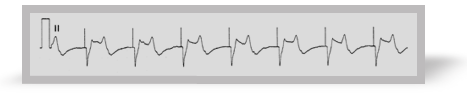
Once the patient is connected to the external pacemaker the output (in milliamps) should be increased until electrical capture is achieved.
Once this has occurred the patient cardiovascular status should be reassessed, starting with the pulse, to ensure electrical capture is associated with mechanical capture.
This ECG shows ventricular capture after each pacing spike.
References
Chapter 10 of the ALS manual has more detail about cardiac pacing and the various pacing methods.
Chapter 11 of the ALS manual has more detail about assessing and treating bradycardia arrhythmias.
Algorithm: Adult bradycardia algorithm