The tachycardia algorithm


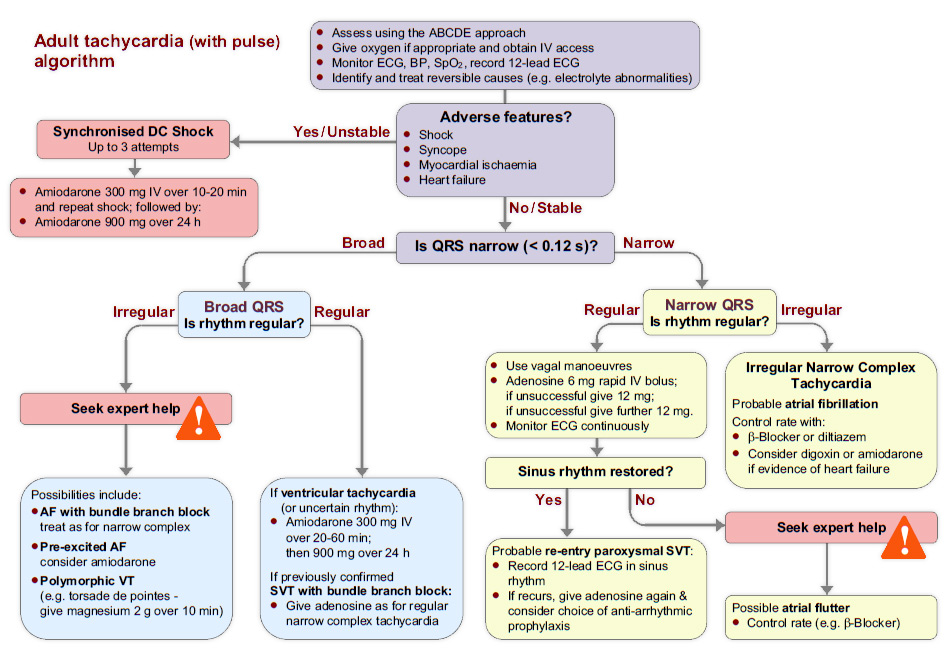
The first step in assessing and treating all deteriorating or critically ill patients is to use the ABCDE approach (Airway, Breathing, Circulation, Disability, Exposure).
Secondly, you should ensure that the following occur:
- Oxygen, if appropriate, is given and IV access is obtained
- Cardiac monitoring is established, and blood pressure and spo2 are recorded
- A 12-lead ECG is recorded at the earliest opportunity
- Reversible causes are identified and treated

The next stage in the tachycardia algorithm is to determine if the patient has any adverse features.
The presence or absence of adverse features will dictate the urgency and choice of treatment for most arrhythmias.
The following adverse features indicate that a patient is unstable and at risk of deterioration:
- Shock
- Syncope
- Heart failure
- Myocardial ischaemia
Roll over the image to enlarge it. Select More to continue.

If the patient does have adverse features this implies that the patient’s condition is unstable and they are at risk of deterioration. So the next course of action is synchronised cardioversion.
If cardioversion fails to terminate the arrhythmia and adverse features persist, administer 300 mg amiodarone IV over 10-20 min and perform a repeat synchronised cardioversion. The loading dose of amiodarone can be followed by an infusion of 900mg over 24 h.
Roll over the image to enlarge it. Select More to continue.
If the patient does not display any adverse features and is stable, the next step is to assess whether the QRS complexes are broad (>0.12 s) or narrow (i.e. normal)
The next stage in the algorithm (for both broad and narrow QRS) will ask you to determine if the patient’s rhythm is regular or irregular.
Roll over the image to enlarge it. Select More to continue.
If the rhythm is irregular and the QRS is broad, you should seek expert help. Possible explanations for this rhythm include:
- Atrial fibrillation (AF) with bundle branch block, which is the most common cause. This should be treated with a ß-blocker (or if this is contra-indicated, diltiazem). If there is evidence of heart failure, digoxin or amiodarone may be more appropriate choices of treatment
- Pre-excited AF (consider amiodarone)
- Polymorphic VT (torsades de pointes – 2 g magnesium should be given intravenously over 10 min)

If the:
- QRS is broad
- Rhythm is regular
A regular broad complex tachycardia may be ventricular tachycardia (VT) or a supraventricular rhythm with bundle branch block. In a stable patient, if there is uncertainty about the origin of the arrhythmia, intravenous adenosine during a multi-lead ECG recording may clarify the nature of the rhythm. This should be done under expert supervision.
Otherwise, treat with amiodarone 300 mg IV, administered over 20 - 60 minutes, followed by a further 900 mg over 24 h.
If the same rhythm in this patient has previously been confirmed to be supraventricular tachycardia (SVT) with bundle branch block, give adenosine IV as first-line treatment, as described for treatment of a regular narrow complex tachycardia.
Roll over the image to enlarge it. Select More to continue.
If the QRS is narrow and the rhythm is regular, in the absence of adverse symptoms you should start with vagal manoeuvres, recording a multi-lead ECG during performance of these.
If the arrhythmia persists and is not atrial flutter, give adenosine 6 mg as a very rapid intravenous bolus, recording a multi-lead ECG during the injection. If there is no response give a 12 mg bolus. If necessary give a further 12 mg dose if there is no response.
If either vagal manoeuvres or adenosine restores sinus rhythm, the rhythm was probably re-entry paroxysmal SVT. You should record a 12-lead ECG in sinus rhythm and can give further adenosine if the arrhythmia recurs. Consider carefully whether or not anti-arrhythmic prophylaxis will be of benefit in the setting of the individual patient. If uncertain, seek expert help.
If sinus rhythm is not restored then you should seek expert help.
Roll over the image to enlarge it. Select More to continue.
If the QRS is narrow and the rhythm is irregular, you are dealing with Irregular Narrow Complex Tachycardia.
In this situation atrial fibrillation is the most likely rhythm. In the absence of adverse features immediate treatment options include:
- Rate control by drug therapy, for example with a ß-blocker
- Rhythm control, using a drug to try to achieve chemical cardioversion
- Rhythm control by synchronised cardioversion
- Treatment to prevent complications
Obtain expert help to determine the most appropriate treatment for the individual patients.
Roll over the image to enlarge it. Select More to continue.
The tachycardia algorithm can be found in chapter 11 of the ALS manual.
It aims to provide a clear and concise diagnosis pathway for use with patients with tachyarrhythmia.
Roll over the image to enlarge it.Select Restart to review the algorithm, or select Menu to return to the main menu.



References

See chapter 11 of the ALS manual for further reading about the tachycardia algorithm.
The 6-stage approach
1. Is there any electrical activity?
2. What is the ventricular (QRS) rate?
3. Is the QRS rhythm regular or irregular?
4. Is the QRS width normal (narrow) or broad?
Any cardiac rhythm can be described accurately and managed safely and effectively using the first four stages.
5. Is atrial activity present? (If so, what is it: Typical sinus P waves? Atrial fibrillation? Atrial flutter? Abnormal P waves?)
6. How is atrial activity related to ventricular activity? (e.g 1:1 conduction, 2:1 conduction, etc, or no relationship)

The tachycardia algorithm
The tachycardia algorithm is available in chapter 11 of the ALS manual.