- Scenario two – analysing the ABG results
![Graphical text that says: Intubated, Ventilated 50% oxygen, Heart rate – 120 min[sup]-1[/sup], BP 150/95mmHg, Comatose GCS 3.](images/m35_t10_025.png)
Feedback
That is not quite right. Have another go.
Feedback
That is not quite right.
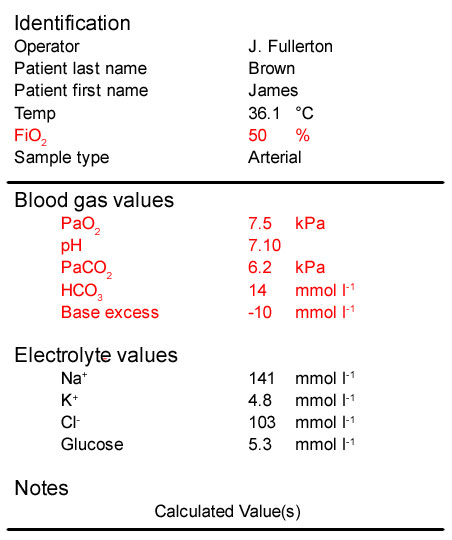
- This patient’s PaO2 is <10kPa which means he is hypoxaemic. We would also expect a much higher PaO[sub]2[/sub] breathing 50% oxygen (approximately 40 kPa), suggesting severely impaired oxygenation
- His pH is 7.10, well below normal confirming that he is acidaemic
- His PaCO[sub]2[/sub] is increased which is consistent with the low pH indicating a respiratory acidosis. However, the severity of the acidosis is unlikely to be due only to the raised PaCO[sub]2[/sub]
- His bicarbonate and base excess are very low and consistent with a metabolic acidosis. They have been consumed to try and buffer the effects of the acids produced by anaerobic respiration during the arrest
In summary:
This is a typical ABG result after prolonged cardiac arrest. There is a mixed metabolic and respiratory acidosis – the predominant component is metabolic, with significant impairment of oxygenation.
Treatment will include:
- Increase the FiO[sub]2[/sub] – this should increase the PaO[sub]2[/sub].
- Increase the minute ventilation to reduce the PaCO[sub]2[/sub] – this will quickly increase the pH.
- Optimise the cardiac output – increased oxygen delivery to the tissues will restore aerobic metabolism, reduce the lactic acidosis and slowly restore the pH towards normal.
- Bicarbonate is not indicated as restoring cardiac output will restore plasma bicarbonate.
Feedback
That is not right. Have another go.
Feedback
That is not right.
- This patient’s PaO2 is <10kPa which means he is hypoxaemic. We would also expect a much higher PaO[sub]2[/sub] breathing 50% oxygen (approximately 40 kPa), suggesting severely impaired oxygenation
- His pH is 7.10, well below normal confirming that he is acidaemic
- His PaCO[sub]2[/sub] is increased which is consistent with the low pH indicating a respiratory acidosis. However, the severity of the acidosis is unlikely to be due only to the raised PaCO[sub]2[/sub]
- His bicarbonate and base excess are very low and consistent with a metabolic acidosis. They have been consumed to try and buffer the effects of the acids produced by anaerobic respiration during the arrest
In summary:
This is a typical ABG result after prolonged cardiac arrest. There is a mixed metabolic and respiratory acidosis – the predominant component is metabolic, with significant impairment of oxygenation.
Treatment will include:
- Increase the FiO[sub]2[/sub] – this should increase the PaO[sub]2[/sub].
- Increase the minute ventilation to reduce the PaCO[sub]2[/sub] – this will quickly increase the pH.
- Optimise the cardiac output – increased oxygen delivery to the tissues will restore aerobic metabolism, reduce the lactic acidosis and slowly restore the pH towards normal.
- Bicarbonate is not indicated as restoring cardiac output will restore plasma bicarbonate.
Feedback
That is right.
- This patient’s PaO2 is <10kPa which means he is hypoxaemic. We would also expect a much higher PaO[sub]2[/sub] breathing 50% oxygen (approximately 40 kPa), suggesting severely impaired oxygenation
- His pH is 7.10, well below normal confirming that he is acidaemic
- His PaCO[sub]2[/sub] is increased which is consistent with the low pH indicating a respiratory acidosis. However, the severity of the acidosis is unlikely to be due only to the raised PaCO[sub]2[/sub]
- His bicarbonate and base excess are very low and consistent with a metabolic acidosis. They have been consumed to try and buffer the effects of the acids produced by anaerobic respiration during the arrest
In summary:
This is a typical ABG result after prolonged cardiac arrest. There is a mixed metabolic and respiratory acidosis – the predominant component is metabolic, with significant impairment of oxygenation.
Treatment will include:
- Increase the FiO[sub]2[/sub] – this should increase the PaO[sub]2[/sub].
- Increase the minute ventilation to reduce the PaCO[sub]2[/sub] – this will quickly increase the pH.
- Optimise the cardiac output – increased oxygen delivery to the tissues will restore aerobic metabolism, reduce the lactic acidosis and slowly restore the pH towards normal.
- Bicarbonate is not indicated as restoring cardiac output will restore plasma bicarbonate.
References
Essentials: 5-step approach to ABG interpretation
Step 2 – is the patient hypoxaemic?
Step 3 – is the patient acidaemic or alkalaemic?
Step 4 – what happened to the PaCO2?
Step 5 – what has happened to the base excess or bicarbonate?
Normal values
PaO[sub]2[/sub] > 10 kPa (75 mmHg) on air
pH 7.35 – 7.45
PaCO[sub]2[/sub] 4.7 – 6.0 kPa
HCO[sub]3[/sub] 22 – 26 mmol l-1
BE +/- 2 mmol l[sup]-1[/sup]