
Indications for ECG monitoring
Choose all the options that are correct and then select Confirm.

That is not quite right.
No, that is still not quite right.
Patients who do require monitoring:
Patient 2; a systolic BP of 60 mm Hg represents shock and there is a high risk of sudden deterioration and death.
Patient 3; even though the myocardial infarction has been uncomplicated, the first complication may be an arrhythmia.
Patient 5; syncope during exercise is a high-risk symptom that may indicate structural heart disease and/or a high risk of life-threatening arrhythmia.
Patients who do not require monitoring:
Patient 1; sinus tachycardia is a common physiological response to anxiety, so this finding alone does not need monitoring in the absence of any other indication of risk, and a family history alone does not indicate this.
Patient 4; sinus bradycardia is a common physiological response to exercise training and does not require monitoring in the absence of any other suspicion of risk.
That is not right.
No, that is still not right.
Patients who do require monitoring:
Patient 2; a systolic BP of 60 mm Hg represents shock and there is a high risk of sudden deterioration and death.
Patient 3; even though the myocardial infarction has been uncomplicated, the first complication may be an arrhythmia.
Patient 5; syncope during exercise is a high-risk symptom that may indicate structural heart disease and/or a high risk of life-threatening arrhythmia.
Patients who do not require monitoring:
Patient 1; sinus tachycardia is a common physiological response to anxiety, so this finding alone does not need monitoring in the absence of any other indication of risk, and a family history alone does not indicate this.
Patient 4; sinus bradycardia is a common physiological response to exercise training and does not require monitoring in the absence of any other suspicion of risk.
Yes, that is right.
Patients who do require monitoring:
Patient 2; a systolic BP of 60 mm Hg represents shock and there is a high risk of sudden deterioration and death.
Patient 3; even though the myocardial infarction has been uncomplicated, the first complication may be an arrhythmia.
Patient 5; syncope during exercise is a high-risk symptom that may indicate structural heart disease and/or a high risk of life-threatening arrhythmia.
Patients who do not require monitoring:
Patient 1; sinus tachycardia is a common physiological response to anxiety, so this finding alone does not need monitoring in the absence of any other indication of risk, and a family history alone does not indicate this.
Patient 4; sinus bradycardia is a common physiological response to exercise training and does not require monitoring in the absence of any other suspicion of risk.



References

See chapter 8 of the ALS manual for further explanation and examples about how to analyse ECG rhythm strips.
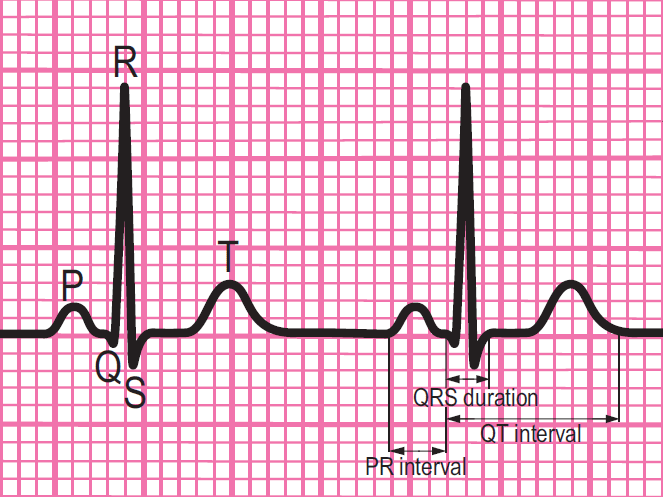
Components of a normal ECG complex
- Depolarisation begins in the SA node and then spreads through to the atrial myocardium
- The heart reacts to this depolarisation. The atrial contraction is recorded on the rhythm strip as the P wave
- The small isoelectric segment between the P wave and QRS complex represents the delay in transmission through the AV node
- Depolarisation of the bundle of His, bundle branches and ventricular myocardium is shown on the rhythm strip as the QRS complex
- The T wave represents recovery of the resting potential in the cells of the conducting system and ventricular myocardium


The 6-stage approach
1. Is there any electrical activity?
2. What is the ventricular (QRS) rate?
3. Is the QRS rhythm regular or irregular?
4. Is the QRS width normal (narrow) or broad?
Any cardiac rhythm can be described accurately and managed safely and effectively using the first four steps.
5. Is atrial activity present? (If so, what is it: Typical sinus P waves? Atrial fibrillation? Atrial flutter? Abnormal P waves?)
6. How is atrial activity related to ventricular activity? (e.g 1:1 conduction, 2:1 conduction, etc, or no relationship)