- Heart block
Extreme bradycardia may sometimes precede cardiac arrest and this may be prevented by prompt and appropriate treatment. In this context the most important bradyarrhythmia is complete heart block.

First degree atrioventricular block
The PR interval is the time between the onset of the P wave and the start of the QRS complex (whether this begins with a Q wave or R wave). The normal PR interval is between 0.12 and 0.20 s (or 3-5 small squares).
First degree atrioventricular (AV) block is present when the PR interval is > 0.20 s and is a common finding. It represents a delay in conduction through the AV junction (the AV node and immediately adjacent myocardium).
First degree AV block rarely causes any symptoms and as an isolated finding rarely requires treatment.

Second degree atrioventricular block
Second degree AV block is present when some, but not all, P waves are conducted to the ventricles, resulting in absence of a QRS complex after some P waves. There are two types.
Mobitz Type I AV block (also called Wenckebach AV block)
The PR interval shows progressive prolongation after each successive P wave until a P wave occurs without a resulting QRS complex. Often the cycle is then repeated.
The need for treatment is dictated by the effect of the bradyarrhythmia on the patient and the risk of developing more severe AV block or asystole.
.")
Mobitz Type II AV block
There is a constant PR interval in the conducted beats but some of the P waves are not followed by QRS complexes.
This may occur randomly, without any consistent pattern. People with Mobitz II AV block have an increased risk of progression to complete AV block and asystole.
2:1 AV block describes the situation in which only alternate P waves are followed by a QRS complex. 2:1 AV block may be due to Mobitz I or Mobitz II AV block and it may be difficult to distinguish which it is from the ECG appearance. If bundle branch block is present (broad QRS complexes) as well as 2:1 block, this is likely to be Mobitz II block.
.")
3:1 AV block
3:1 AV block is less common and is usually a form of Mobitz II AV block.
Immediate decisions about treatment of these rhythms will be determined by the effect of the resulting bradycardia on the patient. After identifying and providing any necessary immediate treatment, continue cardiac monitoring and arrange expert cardiological assessment.
 atrioventricular block.")
Third degree atrioventricular block
In third degree (complete) AV block, there is no relationship between P waves and QRS complexes; atrial depolarisation and ventricular depolarisation arises independently from intrinsic ‘pacemakers’. The site of the pacemaker stimulating the ventricles will determine the ventricular rate and QRS width.
A pacemaker site in the AV node or proximal bundle of His may produce a narrow QRS complex.
A pacemaker site in the distal His-Purkinje fibres or ventricular myocardium will produce broad QRS complexes and is more likely to stop abruptly, resulting in asystole.
Roll over the rhythm strip to see a larger image.
References
See chapter 8 of the ALS manual for further reading about estimating the heart rate, QRS and cardiac arrest rhythms, heart blocks and bradyarrhythmia.
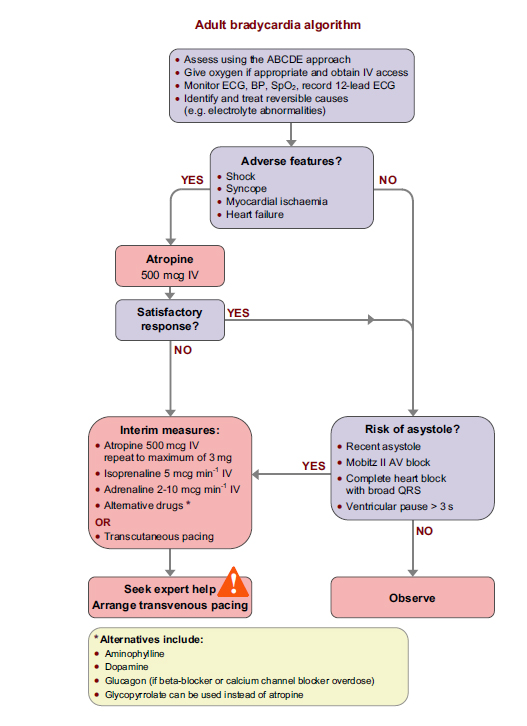
Algorithm: Adult bradycardia algorithm