
Non-ST-segment-elevation myocardial infarction
Click on the red circles to discover more information.


In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.
In some situations the presence of T wave inversion indicates that myocardial damage has occurred or is occurring. T wave inversion may develop, with or without the presence of Q waves, following an ST-elevation MI (STEMI). T wave inversion may also be present as the only abnormality during an acute coronary syndrome, and when accompanied by clinical and biochemical evidence of acute MI but no ST segment elevation, this indicates a non-ST-segment-elevation MI (NSTEMI). However T wave inversion alone is non-specific and may be present in many people for other reasons, so should not be regarded as evidence of acute MI unless there is supportive clinical and biochemical evidence.
On this ECG there is deep T wave inversion in the anterolateral chest leads and in the lateral limb leads (I and aVL) in a patient with clinical features of myocardial infarction. There is no ST segment elevation. This suggests an acute coronary syndrome and the presence or absence of troponin release will indicate whether or not myocardial infarction has occurred. T wave inversion of this nature suggests a high-risk situation, requiring early assessment and treatment by a cardiologist, after the usual initial measures for all acute coronary syndromes.
Click on the red circles to discover more information. Select Next to continue.


References

Acute coronary syndromes: immediate
treatment and components of a normal
ECG rhythm strip
Acute coronary syndromes: immediate treatment
Give immediate treatment to relieve symptoms, limits myocardial damage and reduce the risk of cardiac arrest. Immediate general treatment for ACS comprises:
- Aspirin
- Nitroglycerine
- Oxygen
- Morphine or Diamorphine
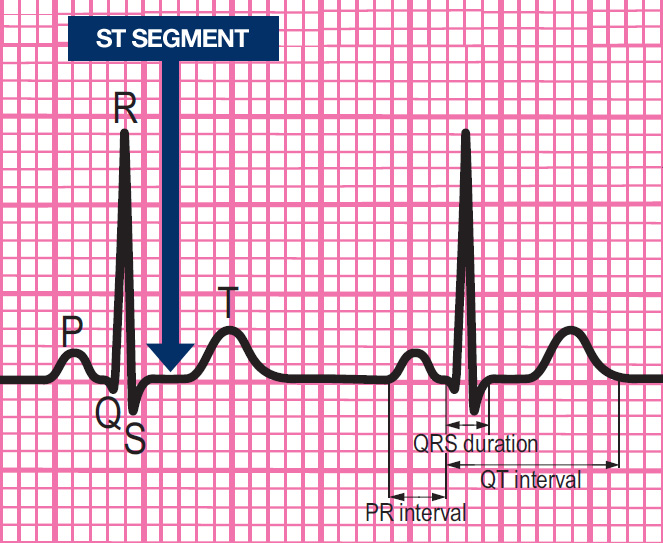
Components of a normal ECG complex
- Depolarisation begins in the SA node and then spreads through the atrial myocardium
- This depolarisation is recorded on the rhythm strip as the P wave. The heart responds to this electrical stimulus byatrial contraction
- The small isoelectric segment between the P wave and QRS complex represents the delay in transmission through the AV node
- Depolarisation of the bundle of His, bundle branches and ventricular myocardium is shown on the rhythm strip as the QRS complex
- The T wave represents recovery of the resting potential (repolarisation) in the cells of the conducting system and ventricular myocardium


The ABCDE approach
All patients with a suspected acute coronary syndrome should be assessed using the ABCDE approach.
